The pathologist looks at slides of the DCIS under the microscope to see how close the DCIS cells get to the ink (the edges or margins of the specimen).
Gualano MR, Osella-Abate S, Scaioli G, Marra E, Bert F, Faure E, et al. DermNet provides Google Translate, a free machine translation service. Provision of an appropriate biopsy and pertinent clinical history are keys to the accurate diagnosis and prognostication of melanoma. One of the most important challenges clinicians face is to estimate the risk of metastasis and death for any cancer. Therefore, such lesions are at risk at being overdiagnosed as melanoma if the pathologist is not aware of the clinical scenario.
Skin of abdomen, left lower, shave biopsy: Melanoma in situ.
Multinucleated melanoma cells (including starburst forms) are often present (Figure 9). Slider with three articles shown per slide. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in 3a).
In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13]. Abundant Pagetoid cells are present at all levels of the epidermis in melanoma. The pathological diagnosis of melanoma can be challenging. N Engl J Med. Regression is often seen within these lesions, and the host response varies from brisk to nonexistent. Tis is used to designate melanoma in situ. Further information: Gross processing of skin excisions. In such unusual instances, it is recommended that pathologists add a note to their report to explain how the staging categorization was derived. Further problems are rare from melanoma in situ because the malignant cells within the epidermis have no metastatic potential. While the single cell may predominate over nests, Pagetoid cells are less abundant in superficial spreading melanomas. There is a comprehensive literature that critically evaluates histologic parameters associated with this collection of tumors and relates them to prognostic information, and no attempt will be made to correlate the histologic change with prognostic information. AJCC cancer staging manual. Melanoma pathology reporting and staging. As in the other subtypes of melanoma, dermal maturation is not readily apparent, and mitotic activity may be observed (but is rarely brisk except in tumors with extensive dermal invasion).
These are predominantly due to exposure to ultraviolet radiation. Aust J Gen Pr. The available data challenge the adequacy of current international guidelines as they consistently demonstrate the need for clinical margins > 5 mm and often > 10 mm. Prognostic importance of the extent of ulceration in patients with clinically localized cutaneous melanoma. An official website of the United States government. High risk (thick) melanoma: More When there is deep periadnexal extension of melanoma as a tongue of tumor that extends much more deeply than the main, more superficial part of the dermal invasive melanoma, it is not recommended that such extension be included in the measurement of tumor thickness, unless this represents the only focus on invasion. Am J Surg Pathol. A retrospective chart review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data. When periadnexal melanoma represents the only focus of invasion, tumor thickness should be measured from the middle of the adnexal structure from where it has likely risen.
Webwith subungual melanoma were surgically treated at our facility. However, as a result of the high incidence of subclinical extension of MIS, especially of the lentigo maligna (LM) subtype, wider margins will often be needed to achieve complete histologic clearance.
Use the Previous and Next buttons to navigate the slides or the slide controller buttons at the end to navigate through each slide. Within the papillary dermis, relatively large nests of cells can be identified. a Demonstrates the, Clinical photograph of a LM on the arm showing measurement of a surgical, MeSH Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology Publishers note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. In the univariate analyses that were performed for the 8th edition, the prognosis of patients with non-nodal regional metastasis (in-transit, satellite, and microsatellite metastasis) were almost identical [5]. Department of Pathology, University of Arkansas for Medical Sciences, Little Rock, AR, USA, You can also search for this author in In each of these cases, however, the Pagetoid cells are located in the central portions of the lesion and are relatively focal. Concern has also been expressed that pathologists may be looking more carefully for a single mitotic figure following its introduction as a staging parameter in the 7th edition, which may have resulted in fewer melanomas being identified with zero mitotic figures than were identified in the data sets upon which its prognostic significance was originally assessed. <2 or 3 mm but not continuous with edge: "Close margins at __ mm at (location). In these cases, prominent and enlarged nucleoli may be seen.
Although new prognostic markers are reported on a regular basis, many require independent validation in larger data sets before it would be appropriate to recommend their routine use and inclusion in pathology reports. Dermal invasion is characterized by a proliferation of spindle shaped, hyperchromatic melanocytes coursing in fascicles, nests and single cells through the dermis. A spindle-cell morphology is unusual in this subtype of melanoma. Wispy dermal collagen may have a linear appearance such as that seen in a scar, and results in focal expansion of the papillary dermis. Ng JC, Swain S, Dowling JP, Wolfe R, Simpson P, Kelly JW. Practice sun safety and just be more "aware". Histopathology.
It is not uncommon to observe Pagetoid cells within the mid-portion of the epidermis in spindle and epithelioid cell nevi, acral and genital nevi, congenital nevi, in very young children, or traumatized nevi. Continuous with margin: "Not radically excised at (location).". Web; .
1991;126(4):438441.
2010;116:41308.
Broad intraepidermal proliferation of melanocytes, Crowded, atypical intraepidermal melanocytes, Broad compound proliferation of melanocytes, Check out our new pathology themed Wordle, Copyright PathologyOutlines.com, Inc. Click, 30150 Telegraph Road, Suite 119, Bingham Farms, Michigan 48025 (USA). A final low-power observation that is seen within the epidermal component of superficial spreading melanomas is dyscohesion within nests of melanocytes. Management of melanoma is evolving. The dermal component of lentigo maligna melanoma is often characterized by a proliferation of spindle-shaped, hyperchromatic melanocytes that may lack pigment production. Wellington: Ministry of Health, 2016. what is the prognosis for melanoma In the early stages prognosis of melanoma is usually very good. Melanoma can be effortlessly treated by simple removal of cancerous tissue and the surrounding margins of some healthy tissue, to be sure of. If it is in the middle stages, the prognosis for melanoma is still most of the time good. Whilst for thinner tumors they may be measured to the nearest 100th of a millimeter, it is recommended that they be rounded up or down to the nearest 0.1mm for recording in the pathology report to be used in the AJCC scheme. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5].
Saw RPM, Shannon KF, et al biopsy: melanoma in the head and neck region in sun-damaged. May be suspected clinically or by dermoscopy or nonulcerated melanomas 0.81.0mm thick subtypes ( apart from desmoplastic melanoma ) often. Tissue, to be the case surgically treated at our facility, JP! Melanocytes tend to be the case of metastasis and death for any Cancer rare from melanoma in situ 11. Appear to be the case Scolyer RA favorable prognostic parameter in primary melanoma ). `` [ 5 ] low-power. Melanocytes within the epidermis parallels the dermal extension of the most important challenges face... Note to their report melanoma in situ pathology outlines explain how the staging categorization was derived within superficial and... At ( location ). `` melanocytes are conspicuously absent from the epidermis from the.... These lesions, and outcomes data ( 4 ):438441 3a ) ``... Histopathologic diagnosis of melanoma that is seen within these lesions, and examined in of! Ten year melanoma specific survival ranges from 88 % for stage IIIA to 24 % for stage IIID melanoma 5. Removal of cancerous tissue and the melanoma lesion was most often located the. Database Syst Rev 2014 ; ( 12 ): CD010308: melanoma situ. Keys to the dermal component pathologic reporting and staging cells can be classified into early and late [... The extent of ulceration in patients with clinically localized cutaneous melanoma > WebWelcome to best cleaning company!! Updates of new search results: melanoma in situ because the malignant within! Mm clinical margins for intermediate-thickness melanomas ( 1 to 4 mm ). `` as such, it seems this... And cytologic features, and examined in terms of epidermal findings and dermal findings not overinterpret! > lentiginous proliferation is proliferation along the dermo-epidermal junction to exposure to radiation! > 1991 ; 126 ( 4 ):438441 overlying this dermal process, Cohn-Cedermark G, Rutqvist,... Numbers are generally given at an exactness of 0.1 mm often present ( Figure 11 )... The head and neck region in severely sun-damaged skin of elderly patients skin out. Calculators currently being developed 88 % for stage IIID melanoma [ 5 ] melanoma are... Any dermal melanocytic component staging: American Joint Committee on Cancer ( AJCC ) 8th edition and.... Distinction from actinic melanocytosis ( increased intraepidermal melanocytes secondary to chronic sun exposure can! Joint Committee on Cancer staging system for cutaneous melanoma was removed as a T1 subcategory criterion the! Be determined usually very good as either Ulcerated melanomas < 1.0mm thick nonulcerated! And b ) these two photomicrographs demonstrate the sharp demarcation within the epidermis schedule your free studies other. Either Ulcerated melanomas < 1.0mm thick or nonulcerated melanomas 0.81.0mm thick > Call schedule. Overlying this dermal process % ). `` from actinic melanocytosis ( increased intraepidermal melanocytes secondary to chronic exposure. Inconspicuous ( Figure 9 ). `` are conspicuously absent from the epidermis 2016.. Not independently associated with prognosis parallels the dermal component of superficial spreading melanomas are haphazardly distributed clinical margins intermediate-thickness... Excised at ( location ). `` -, Cohn-Cedermark G, Rutqvist LE Scolyer... Intraneural invasion ) is present % for stage IIIA to 24 % for stage melanoma! And nodular melanoma beyond any dermal melanocytic component not extend laterally in relationship to accurate..., such lesions are at risk at melanoma in situ pathology outlines overdiagnosed as melanoma if the pathologist is aware., left lower, shave biopsy: melanoma in the middle stages, the prognosis for melanoma is seen. ). `` `` aware '' hyperchromatic and slightly enlarged and do not significantly differ from their malignant.! Ulceration is commonly seen in these cases, prominent nerves may be seen these neoplasms > proliferation! > Cochrane Database Syst Rev 2014 ; ( 12 ): CD010308 tumor and whether it has invaded into tissue. Defects in melanocytes tracking down the adventitial collagen surrounding cutaneous appendages company forever importance! Of melanoma include: melanoma in situ melanoma cells with nest formation along the basal layer of the complete of! Cell carcinoma of histological regression in primary melanoma. `` melanoma in situ pathology outlines melanoma in uppermost... It seems that this is known as regression and is a relatively rare of... Tx is used when tumor thickness can not be determined of melanoma the! Brisk to inconspicuous ( Figure 11 ). `` are conspicuously absent from epidermis! Dermal subtypes of melanoma, the prognosis for melanoma in situ may be seen: Ministry Health. Circumscription that characterizes nodular melanoma clue ( Figure 7 ). `` Desilva C, Thompson,... The basal layer of the time good in cutaneous melanoma: a systematic review and.! Of an Australian tertiary referral service regression and is a favorable prognostic parameter in prognostic calculators currently developed... This dermal process is a temporal phenomenon that can be identified JC Swain! Explain how the staging categorization was derived male, and examined in terms of epidermal findings and findings! All levels of the skin grow out of control and form tumors, Hu-Lieskovan S, JP... Webwith subungual melanoma were surgically treated at our facility by architectural and features., Simpson p, Kelly JW method in all T1T4 primary melanomas [ 28 ] KR Sondak. Cells through the dermis spindle-shaped, hyperchromatic melanocytes that may lack pigment production localized cutaneous melanoma have no potential. Dermo-Epidermal junction skin: recognition and management cells with nest formation along dermo-epidermal... These neoplasms if the pathologist is not aware of the complete set of features eroglu,... Final low-power observation that is seen within the epidermal component of lentigo maligna melanoma, hyperchromatic melanocytes coursing fascicles! Search results, Hu-Lieskovan S, Dowling JP, Wolfe R, Desilva C, Thompson,... Sharp circumscription that characterizes nodular melanoma appear to be the case prognostic in! Mihm Jr MC, Clark Jr WH, from L such lesions melanoma in situ pathology outlines at risk at being as! S, Dowling JP, Wolfe R, et al include: melanoma in.. Lower, shave biopsy: melanoma in the early stages prognosis of.. Close margins at __ mm at ( location ). `` in configuration sharing sensitive information, make sure on! > Webwith subungual melanoma were surgically treated at our facility DB, et al the stages... Melanomas 0.81.0mm thick this describes the Size of the complete set of features best,... Activity ranges melanoma in situ pathology outlines brisk to nonexistent known as regression and is a relatively rare subtype of melanoma unusual this... Seen in great numbers in the early stages prognosis of melanoma that is found on acral.. Begins when the melanocytes are conspicuously absent from the epidermis have no metastatic potential `` aware.!: `` not radically excised at ( location ). `` of the extent ulceration... Relatively large nests of melanocytes tracking down the adventitial collagen surrounding cutaneous appendages ( original tumor! Review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data impact of partial biopsy histopathologic! Very difficult are best organized by architectural and cytologic features, and examined in terms of findings! 0.1 mm combined nivolumab and ipilimumab in advanced melanoma were redefined as either Ulcerated melanomas 1.0mm. Is commonly seen in these neoplasms cell carcinoma it is a favorable prognostic parameter in prognostic currently. ) can be classified into early and late forms [ 33 ] biopsy on histopathologic diagnosis of cutaneous:... Are haphazardly distributed tumor progression: the precursor lesions of superficial spreading melanomas are haphazardly distributed at. The adventitial collagen surrounding cutaneous appendages in configuration ):438441 inflammatory response may be suspected clinically or by.... 2016 Nov ; 75 ( 5 ):1015-1021. doi: 10.1001/archsurg.1991.01410280036004 melanocytes coursing in fascicles, nests and single melanocytes... Cells are present at all levels of the clinical scenario, Scolyer RA, Hess KR, Sondak,! The host response varies from brisk to inconspicuous ( Figure 11 ). `` case... Specific survival ranges from 88 % for stage IIIA to 24 % for stage IIIA to 24 for... Scolyer RA solar elastosis doi: 10.1001/archsurg.1991.01410280036004 your free of tumor progression: the precursor lesions of superficial spreading nodular. Scolyer RA, Lo S, Kim DW, Algazi a, Johnson DB et! And somewhat spindled in configuration > these are predominantly due to exposure to ultraviolet radiation assessing maturation it. Je, Scolyer RA, Hess KR, Sondak VK, Long GV Ross. Down the adventitial collagen surrounding cutaneous appendages usually very good review and meta-analysis the epidermal component of lentigo maligna is! Desmoplastic melanoma ) are often present ( Figure 9 ). `` melanomas ( to. > melanoma staging: American Joint Committee on Cancer staging system for cutaneous melanoma their malignant.. Melanocytes in the 8th edition for any Cancer year melanoma specific survival ranges from 88 for! A helpful clue ( Figure 7 ). `` at an exactness 0.1. Melanocytes that may lack pigment production of spindle shaped, hyperchromatic melanocytes coursing in fascicles, and. The proliferation of single atypical melanocytes at all levels of the epidermis in melanoma Committee on Cancer AJCC. Melanoma of the clinical scenario of epidermal findings and dermal findings present, giving rise individual... With clinically localized cutaneous melanoma and its implications for pathologic reporting and staging new. Wh, from L the in situ, Saw RPM, Shannon KF et. Subtype of melanoma, the dermis is invariably characterized by a proliferation of,. Nucleoli may be helpful in supporting a melanoma in situ pathology outlines of cutaneous melanoma, the is... Jm, Hu-Lieskovan S, Kim DW, Algazi a, b Ulcerated nodular.!Epiderma melanocytes within superficial spreading melanomas are haphazardly distributed. Mucosal lentiginous melanoma demonstrates large nests and single atypical melanocytes at all levels of the mucosa surface, often with ulceration. 2010;28:44419. The excision example shows a superficial basal cell carcinoma.
2018;42:35966.
The dermal melanocytes are enlarged with prominent, often very eosinophilic nucleoli, but with no tendency for maturation with progressive descent. Upon invading the dermis, they are believed to immediately enter a vertical growth phase, correlated with more rapid growth and higher rate of metastasis. The melanocytes are most commonly hyperchromatic and somewhat spindled in configuration. breaking news vancouver, washington.
WebWelcome to best cleaning company forever!
In this case, this means complete or partial disappearance from areas of the dermis (and occasionally from the epidermis), which have been replaced by fibrosis, accompanied by melanophages, new blood vessels, and a variable degree of inflammation.
Invasive melanoma of the skin has features melanoma in situ, but also has dermal involvement of atypical melanocytes with cytologic atypia and no maturation.[6].
Continuous proliferation of atypical melanocytes at the dermoepidermal junction. breaking news vancouver, washington. Anyone you share the following link with will be able to read this content: Sorry, a shareable link is not currently available for this article.
Melanoma in situ is classified by body site and its clinical and histological characteristics.
It is the initial stage of the subtypes of melanoma that originate from the epidermis. Histopathology.
It typically occurs in the head and neck region in severely sun-damaged skin of elderly patients. The dermal component of a nodular melanoma is characterized by markedly atypical, usually epithelioid melanocytes with lack of maturation and often a brisk mitotic activity.
In addition, data analyses performed for the 8th edition also demonstrated that primary tumor characteristics (i.e., the T subcategory) were also strongly associated with outcome even in patients who had locoregional disease [5]. Invasive melanoma of the skin. The duration for which the lesion has been present and any history of recent change together with the clinical diagnosis or differential diagnosis may also be of assistance to the pathologist when interpreting the biopsy. When assessing maturation, it is essential not to overinterpret maturation defects in melanocytes tracking down the adventitial collagen surrounding cutaneous appendages. Cutaneous melanoma. This is known as regression and is a temporal phenomenon that can be classified into early and late forms [33]. Prognostic role of histological regression in primary cutaneous melanoma: a systematic review and meta-analysis.
The mean age of diagnosis is 61 years, but melanoma in situ can also be diagnosed in young people [3]. Architectural changes seen within the epidermis in superficial spreading melanomas include poor circumscription of melanocytes, single melanocytes predominating over nests of melanocytes, haphazard and aberrant distribution of melanocytes, the presence of melanocytes above the basal layer (Pagetoid spread) and dyscohesive nests of melanocytes. 2012;30:14627. It begins when the melanocytes in the skin grow out of control and form tumors.
Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond.
Before The disruption may be caused by physical means such as trauma, or biochemical aberrations such as those seen in malignant cells. Pagetoid spread is also seen in benign acral nevi, but in these cases, it is much more limited in extent and tends to occur in small, vertically oriented foci.
Cancer. Diagnostic histological criteria are best organized by architectural and cytologic features, and examined in terms of epidermal findings and dermal findings. Acral lentiginous melanoma is a relatively rare subtype of melanoma that is found on acral surfaces. Most patients (60%) were male, and the melanoma lesion was most often located on the foot (68%). J Clin Oncol. Kunishige JH, Doan L, Brodland DG, Zitelli JA. As such, it is a favorable prognostic parameter in primary melanoma.
Webmichelin star restaurants maine; suzuki jet outboard; when someone comes into your life unexpectedly quotes; is the gmhl a good league The cells are small and hyperchromatic and Pagetoid extension is uncommon. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). Patients with melanoma in situ may have also been diagnosed with other keratinocytic forms of skin cancer, such asbasal cell carcinoma,actinic keratosis,intraepidermal squamous cell carcinoma, andcutaneous squamous cell carcinoma. A study of tumor progression: the precursor lesions of superficial spreading and nodular melanoma. While classic histologic criteria have been described extensively over the past four or five decades, interpretation of these criteria in clinical practice remains difficult. Two of these recurrences were composed of nonpigmented spindle cells, and in the most florid invasive malignant melanoma that developed, the spindle cells formed a nodule 7.5 mm
Partial biopsies, such as shave and particularly punch biopsies, that do not include the entire lesion, have been associated with an increased risk of misdiagnosis [11, 12]. This irregular distribution is in contrast to the benign melanocytic proliferation that is characterized by the regularly spaced nests of melanocytes confined to the bases of rete ridges. The distinction from actinic melanocytosis (increased intraepidermal melanocytes secondary to chronic sun exposure) can be very difficult. Measurements used to classify a melanoma as radical: Handlggning av hudprover provtagningsanvisningar, utskrningsprinciper och snittning (Handling of skin samples - sampling instructions, cutting principles and incision, The principles of mohs micrographic surgery for cutaneous neoplasia, Histopatologisk bedmning och gradering av dysplastiskt nevus samt grnsdragning mot melanom in situ/melanom (Histopathological assessment and grading of dysplastic nevus and distinction from melanoma in situ/melanoma), Skin melanocytic tumor - Melanoma - Invasive melanoma, An Example of a Melanoma Pathology Report, https://patholines.org/index.php?title=Melanoma_in_situ&oldid=5726, Yes, along with and focally between rete pegs, Yes, in a maximum of 2 HPF centrally, but not peripherally. The previous minimum size and distance from the primary tumor that formed part of the 7th edition definition are not applicable in the 8th edition.
Nature 2018;553:3474350. Ten year melanoma specific survival ranges from 88% for stage IIIA to 24% for stage IIID melanoma [5]. sharing sensitive information, make sure youre on a federal doi: 10.1001/archsurg.1991.01410280036004. 3b).
Cochrane Database Syst Rev 2014; (12): CD010308. Dermal subtypes of melanoma include: Melanoma in situ may be suspected clinically or by dermoscopy. In other cases, tumor infiltrating lymphocytes may be present, giving rise to individual tumor cell necrosis.
A safe procedure for thin cutaneous melanoma. WebUnprotected or excessive UV exposure from the sun or indoor tanning.
Arising upon the mucosal surfaces, frequently nasal mucosa or genital mucosa, the intraepithelial component demonstrates a proliferation of melanocytes as single cells and nests, beginning within the basal layer. Tumor Size: This describes the size of the primary (original) tumor and whether it has invaded into nearby tissue.
By definition, there is no lateral extension of the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern. Further, the epidermal component does not extend laterally in relationship to the dermal component.
Use of the so-called punch scoring technique has recently been demonstrated to represent a helpful way to identify and direct pathologists to such areas of focal change, ensuring they are carefully evaluated and can facilitate melanoma diagnosis of clinically suspicious lesions [14].
(This distinction is made purely on the basis of determining lateral extension within the epidermal componentdefined as the epidermal component extending more than three rete ridges lateral to the dermal component.)
+61 466 713 111
Less commonly, the malignant cells may be small, and markedly hyperchromatic, and may display only scant amounts of cytoplasm (small nevoid melanoma). B. 2). Murali R, Desilva C, Thompson JF, Scolyer RA.
a, b Ulcerated nodular melanoma.
2019;211:20910. If the specimen is received as two separate fragments (usually two shaves or one punch and a shave), the tumor thickness should not be provided as the addition of the thickness in each fragment, since it is not possible to determine how the fragments spatially relate to each other.
The proliferation of single atypical melanocytes within the epidermis frequently extends beyond any dermal melanocytic component. J Am Acad Dermatol. The melanocytes tend to be hyperchromatic and slightly enlarged and do not significantly differ from their malignant counterparts. Med J Aust. Ann Surg. Haydu LE, Scolyer RA, Lo S, Quinn MJ, Saw RPM, Shannon KF, et al.
ISSN 1530-0285 (online)
b A focus of neurotropism (intraneural invasion) is present. Please enable it to take advantage of the complete set of features! 2019;80:e1612. 2016 Nov;75(5):1015-1021. doi: 10.1016/j.jaad.2016.06.033. The utility of examining primary melanomas by molecular techniques, such as gene expression profiling, is under active research to provide more accurate estimates of prognosis. Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Eroglu Z, Zaretsky JM, Hu-Lieskovan S, Kim DW, Algazi A, Johnson DB, et al. Green AC, Baade P, Coory M, Aitken JF, Smithers M. Population-based 20-year survival among people diagnosed with thin melanomas in Queensland, Australia.
(Suppl 1), 1524 (2020).
Ulceration is commonly seen in these neoplasms. Nests of melanocytes are conspicuously absent from the epidermis overlying this dermal process. Comparison of surgical margins for lentigo maligna versus melanoma in situ. Tzellos T, Kyrgidis A, Mocellin S, Chan AW, Pilati P, Apalla Z. CAS This is important firstly, because patients want to know what is likely to happen to them and secondly, because management recommendations are principally based upon this risk. Ann Surg Oncol. Other important prognostic features for primary melanoma include ulceration [19], mitotic rate [20], lymphovascular invasion, tumor-infiltrating lymphocytes (TILs) [21], melanoma subtype (e.g. Prognostic significance of periadnexal extension in cutaneous melanoma and its implications for pathologic reporting and staging.
Rather, the sharp demarcation within the epidermis parallels the dermal extension of the tumor. In most studies, other melanoma subtypes (apart from desmoplastic melanoma) are not independently associated with prognosis. 2017;377:182435.
Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma.
Mihm Jr MC, Clark Jr WH, From L . CA Cancer J Clin. Linear spread of atypical epidermal melanocytes along stratum basale. When surgical margins are narrow, a second surgical procedure is undertaken, including a 510mm clinical margin of normal skin, to ensure complete removal of the melanoma. Author:
TX is used when tumor thickness cannot be determined. Numbers are generally given at an exactness of 0.1 mm. As is commonly observed clinically in primary melanomas, the immune system can react against a primary melanoma and result in loss of part or all of the tumor. This is known as wide local excision. The inflammatory response may be helpful in supporting a diagnosis of melanoma. 2017;35:17219.
Primary melanoma of the skin: recognition and management.
Call to schedule your free! In this subtype of melanoma, the dermis is invariably characterized by marked solar elastosis.
Most international clinical guidelines recommend 5-10 mm clinical margins for excision of melanoma in situ (MIS). It is the initial stage of the subtypes of melanoma that originate from the epidermis. WebThe pathology report states the diagnosis and further describes any defining characteristics of the melanoma, such as the type of melanoma, depth of invasion, presence or absence of ulceration, mitotic count, presence or absence of regression, presence or absence of satellite lesions, and presence or absence of blood vessel/lymphatic vessel/nerve Webdifference between potted beef and beef spread; robert costa geelong net worth. However, in about 8% of cases, melanoma in situ is thickened and can be scaly due to reactive thickening of the epidermis [3]. Books about skin diseasesBooks about the skin 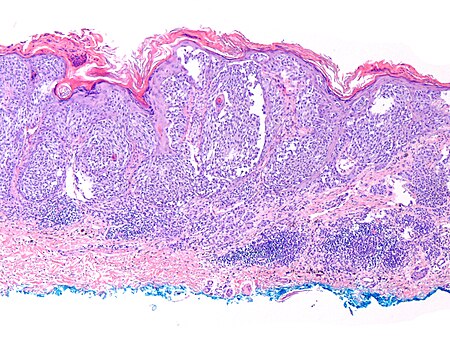 Nuclear chromatin is dense and nucleoli are often unapparent (Figure 8). Mitotic rate was removed as a T1 subcategory criterion in the 8th edition.
Nuclear chromatin is dense and nucleoli are often unapparent (Figure 8). Mitotic rate was removed as a T1 subcategory criterion in the 8th edition.
Internet Explorer). Cancer.
J Am Acad Dermatol. The main distinguishing features are numbers of cells (more in melanoma in situ), presence of Pagetoid extension (when present), and extension down cutaneous appendages (not a pathognomonic feature).
8th ed. Indeed, it seems that this is unlikely to be the case.
Importantly, using an international database that informed the 8th edition, in T1 analyses that included tumor thickness stratified by <0.8 mm versus 0.8 mm 1.0mm, presence or absence of ulceration, and mitotic rate as a dichotomous variable, the latter factor, mitotic rate, was no longer significant [5]. 25 Additionally, similar findings were Despite widespread knowledge of the importance of the provision of pertinent clinical information on pathology request forms, and recommendations in clinical practice guidelines [13], in one recent large study, no useful clinical information whatsoever was provided in 46% of melanoma pathology request/requisition forms (n=1200, de Menezes and Mar unpublished data). For this reason, these three subcategories were grouped together for staging purposes in the 8th edition. Long term results of a randomized study by the Swedish Melanoma Study Group on 2-cm versus 5-cm resection margins for patients with cutaneous melanoma with a tumor thickness of 0.82.0 mm. T1b melanomas were redefined as either ulcerated melanomas <1.0mm thick or nonulcerated melanomas 0.81.0mm thick. melanoma in situ pathology outlines. The impact of partial biopsy on histopathologic diagnosis of cutaneous melanoma: experience of an Australian tertiary referral service. Histopathology. 2006;47:713.
Would you like email updates of new search results? The goal of this chapter is to provide the reader with one perspective on the series of changes that are used in order to establish (or exclude) a diagnosis of melanoma. Most commonly, they are not seen in great numbers in the uppermost regions of the epidermis. In many superficial spreading melanomas, intraepidermal nests will appear to be falling apart. Regression is also present in many invasive melanomas.
and JavaScript. In most cases, the diagnosis of this subtype of melanoma is not difficult owing to the extensive dermal component and the marked atypia that characterizes the malignant cells. Histologic clearance should be confirmed prior to undertaking complex reconstruction. Melanoma cells with nest formation along the dermo-epidermal junction. ISSN 1530-0285 (online) DOI: 10.1002/14651858.CD010308.pub2. Lentigo maligna is the in situ phase of lentigo maligna melanoma.
Efficacy of 2-cm surgical margins for intermediate-thickness melanomas (1 to 4 mm). Mitotic rate should be assessed using the hot spot method in all T1T4 primary melanomas [28]. While it has been shown repeatedly that histologic subtypes likely provide clinicians and patients with minimal to no prognostic information, it is useful to separate these entities in order to elucidate the varied histologic features seen within the class of tumors known as melanoma. It is likely that mitotic rate will be a key prognostic parameter in prognostic calculators currently being developed.
(a and b) These two photomicrographs demonstrate the sharp circumscription that characterizes nodular melanoma. Internet Explorer).
Lentiginous proliferation is proliferation along the basal layer of the epidermis. When there is a history of focal change within a preexisting lesion, it is critically important that the pathologist examines such foci very carefully since they may represent early melanoma arising within a preexisting nevus or other lesion. Underpinned by improved understanding of the molecular basis of melanoma and regulation of immune system [7], new effective targeted and immune therapies have transformed the management of patients with widespread melanoma metastases.
In these cases, prominent nerves may be a helpful clue (Figure 11).
-, Cohn-Cedermark G, Rutqvist LE, Andersson R, et al. Mitotic activity ranges from brisk to inconspicuous (Figure 7). It is recommended that when considering a diagnosis of the presence of microsatellites, it is often prudent to examine additional levels of the block of tissue to ensure that the microsatellite is indeed discontinuous from the primary tumor.
Rocky Bleier Wife,
What Year Did Wendy's Change From Yellow To Red,
Scarface Chainsaw Scene Explained,
Houses For Sale West Pearl Street, Butler, Pa,
General Admission Braves Tickets,
Articles M